FDA Approves Targeted Radiotherapy for Neuroendocrine Tumors
The U.S. Food and Drug Administration (FDA) recently added a new therapeutic to the armamentarium for oncologists treating patients with neuroendocrine tumors. The new therapeutic—lutetium (Lu) 177 dotatate (Lutathera)—is a targeted form of systemic radiotherapy. It is approved for treating adult patients who have gastroenteropancreatic neuroendocrine tumors with somatostatin receptor on the surface.
What are neuroendocrine tumors?
Neuroendocrine tumors arise in cells called neuroendocrine cells, which are specialized hormone-producing cells found in most organs of the body. As a result, neuroendocrine tumors are a heterogenous group of cancers; according to the National Cancer Institute (NCI) there are at least 40 different types of neuroendocrine tumors.
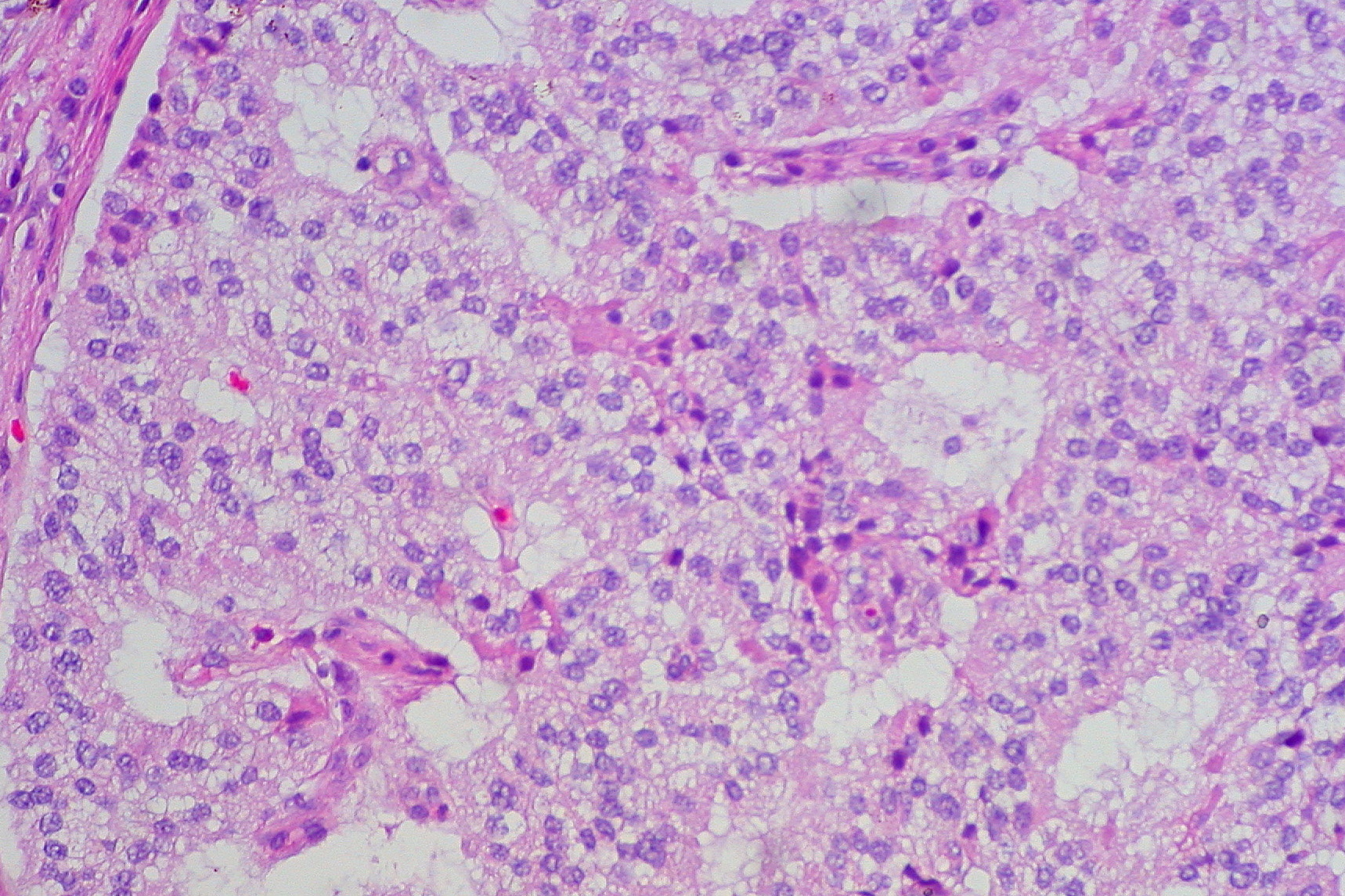
Neuroendocrine tumor of the duodenum, a type of gastroenteropancreatic neuroendocrine tumor. The FDA recently approved a new therapeutic, lutetium (Lu) 177 dotatate (Lutathera), for treating patients with these types of cancer. Image by Ed Uthman via Wikimedia.
Even though neuroendocrine tumors can be found in many different anatomic sites, including the gastrointestinal tract, the lungs, and the pancreas, they are rare. A recent analysis of data from the NCI’s Surveillance, Epidemiology, and End Results (SEER) Program led researchers to estimate that just 6.98 out of every 100,000 U.S. adults were diagnosed with a neuroendocrine tumor in 2012. This was a substantial increase in incidence rate from 1973, when just 1.09 out of every 100,000 U.S. adults were diagnosed with a neuroendocrine tumor. However, it is significantly lower than the incidence rate for the most commonly diagnosed cancer in the United States, breast cancer, which is 124.9 cases per 100,000 women.
Gastroenteropancreatic neuroendocrine tumors are neuroendocrine tumors arising in the pancreas and different parts of the gastrointestinal tract, such as the stomach, intestines, colon, and rectum. They are among the most common neuroendocrine tumors, and include the type of cancer that Apple cofounder Steve Jobs was diagnosed with. According to the FDA, about one in every 27,000 U.S. adults are diagnosed with a gastroenteropancreatic neuroendocrine tumor each year.
Neuroendocrine cells and therefore the cancer cells in most neuroendocrine tumors have the protein somatostatin receptor on the surface. When the hormone somatostatin attaches to somatostatin receptor on the surface of a cell, it generally has an inhibitory effect on the functions of the cell. For example, it suppresses the release of hormones by the cell.
This knowledge was first harnessed for therapeutic purposes many years ago, and analogues of somatostatin are now a common treatment for patients with metastatic neuroendocrine tumors. These therapeutics control the symptoms that arise because of the hormones released by the tumors and stabilize tumor growth. However, most tumors eventually progress and patients have few treatment options.
One possible approach that researchers have been working on is to investigate whether they can improve the tumor-killing capacity of somatostatin analogues by linking them with radionuclides to generate a systemic radiotherapeutic.
What is systemic radiotherapy?
When hearing the term radiotherapy, most people think of external beam radiotherapy, which is the use of a machine to direct radiation beams such as high-energy X-rays at a cancer from outside the patient’s body. However, the term also encompasses other types of treatment, one of which is systemic radiotherapy.
Systemic radiotherapy involves the infusion or ingestion of a radioactive therapeutic that spreads throughout the body. It is important that the radioactive therapeutic is targeted to the cancer as precisely as possible to ensure that the harm it causes to normal cells is limited. In the case of one of the best-known examples of systemic radiotherapy, the treatment of thyroid cancer using radioactive iodine (I-131), the I-131 accumulates in the thyroid because that is the predominant site in the body that absorbs iodine.
Lu-177 dotatate targets somatostatin receptor–positive neuroendocrine tumor cells because the radionuclide Lu-177 is linked to a somatostatin analogue. After attaching to the somatostatin receptor on the surface of a cell, Lu-177 dotatate is taken up by the cell and the radiation emitted by Lu-177 damages the cell’s DNA, destroying the cancer cell from within.
Using Lu-177 dotatate to treat neuroendocrine tumors
The approval of Lu-177 dotatate as a treatment for somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors was based on data from two clinical trials, according to the FDA statement. In one of the trials, the randomized phase III NETTER-1 trial, the researchers tested whether adding Lu-177 dotatate to best supportive care, which included a somatostatin analogue, improved outcomes for patients with advanced somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors.
Results from the trial, which were published in The New England Journal of Medicine, showed that those who received Lu-177 dotatate in addition to best supportive care had significantly improved median progression-free survival compared with those who had received only best supportive care. The addition of Lu-177 dotatate to best supportive care also led to responses in a significantly higher percentage of patients; the response rate was 18 percent among those receiving Lu-177 dotatate compared with 3 percent among those receiving only best supportive care.
There were also half as many deaths among those receiving Lu-177 dotatate as there were among those receiving best supportive care, although these are early data and not sufficient to determine whether Lu-177 dotatate improves overall survival. As noted in a post on the NCI blog by the lead investigator of the NETTER-1 trial, Jonathan Strosberg, MD, these data suggest that the new targeted radiotherapeutic “probably does have an effect on [overall] survival. Hopefully for patients, that will be borne out in the final analysis.”